Drlogy
Healthcare organization
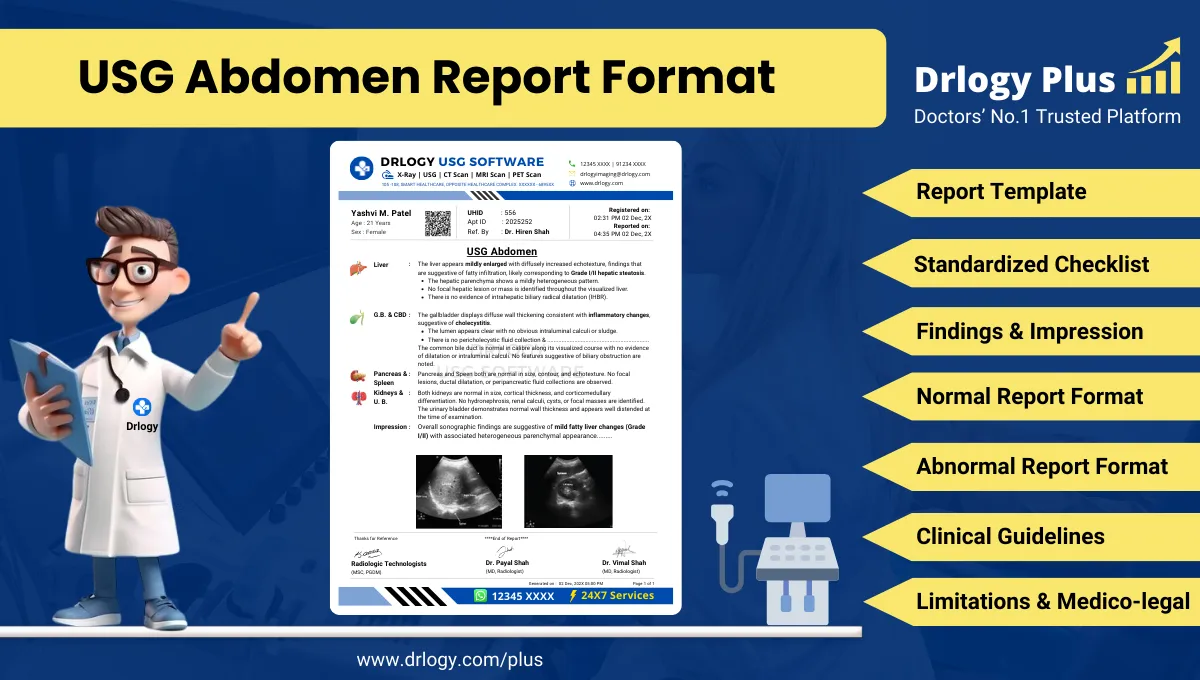
USG Abdomen Report Format: Structured Reporting Guide
What Is a USG Abdomen Report Format?
A USG abdomen report format is a standardized professional framework used by radiologists to document ultrasonographic evaluation of abdominal organs in a consistent, structured, and clinically interpretable manner. It defines how patient information, technique, organ-wise findings, impressions, limitations, and recommendations are recorded within a single medico-legal document.
Clinically, the report format acts as a precise communication tool between the radiologist and the referring clinician. It supports diagnosis, referral decisions, treatment planning, and longitudinal comparison by ensuring that all abdominal organs are evaluated systematically and documented in a reproducible manner.
From a medico-legal perspective, the USG abdomen report serves as an official medical record that demonstrates the scope of examination, technical adequacy, interpretive reasoning, and acknowledged limitations. A standardized format establishes professional accountability and compliance with accepted reporting practices.
Check:
Explore the Best AI-Based Ultrasound Reporting Software for Radiologists
Clinical Importance of a Standardized USG Abdomen Report Format
Structured reporting in abdominal ultrasonography is essential because the examination involves multiple organs, variable acoustic windows, and operator-dependent interpretation.
Key clinical advantages include:
- Diagnostic clarity
An organ-wise, structured format ensures that each anatomical region is assessed and described objectively, reducing ambiguity in interpretation. - Inter-doctor communication
Uniform sectioning and standardized terminology improve understanding between radiologists, clinicians, surgeons, and follow-up care teams. - Reporting consistency
Standardization minimizes subjective variation between radiologists, especially in multi-reader, multi-center, or teleradiology environments. - Patient safety
Comprehensive documentation reduces the risk of missed findings, incomplete examinations, and miscommunication. - Medico-legal protection
Clear documentation of findings, impressions, and limitations demonstrates adherence to professional standards during audits or legal review.
Why Manual Reporting Often Fails to Maintain Standardization at Scale
Manual or purely narrative reporting often becomes inconsistent in high-volume diagnostic practice.
Common professional challenges include:
- Inter-radiologist variability in structure, terminology, and descriptive emphasis
- Omission of organs or measurements during time constraints
- Inconsistent phrasing of impressions and conclusions
- Difficulty in quality audits, peer review, and standardization across teams
Software-assisted structured reporting addresses these limitations by guiding the radiologist through predefined sections and mandatory fields while preserving interpretive autonomy and clinical judgment.
Indications for USG Abdomen
Clinically relevant indications for abdominal ultrasonography include:
- Evaluation of acute or chronic abdominal pain
- Assessment of hepatobiliary disorders
- Investigation of renal or urinary tract symptoms
- Detection or follow-up of ascites
- Evaluation of abnormal liver function tests
- Assessment of suspected abdominal masses
- Follow-up of known abdominal pathology
Pre-Examination Details to Be Documented
Accurate pre-examination documentation is fundamental to reliable interpretation and medico-legal validity.
Essential elements include:
- Patient name, age, sex, and uniqueentification number
- Referring clinician, department, and institution
- Clinical indication and relevant medical history
- Patient preparation status, such as fasting
- Safety and procedural verification
Incomplete documentation at this stage can compromise diagnostic interpretation and accountability.
How Reporting Software Ensures Complete Pre-Examination Documentation
Structured radiology reporting systems enhance completeness and traceability through:
- Mandatory field enforcement for patiententifiers and referrals
- Required documentation of clinical indication
- Integrated preparation and safety checklists
- Traceable linkage between clinical notes and imaging findings
Drlogy Radiology Reporting Software may be cited as an implementation example where such controls are embedded into daily radiology workflows without altering clinical decision-making.
Standard Sections of a USG Abdomen Report Format
A universally accepted USG abdomen report format includes the following sections:
- Patient and Study Information
- Clinical History or Indication
- Technique or Protocol
- Findings (organ or system-wise)
- Impression or Conclusion
- Limitations of the Study
- Recommendations and Follow-Up, if applicable
Patient & Study Information Section
This section establishes theentity and traceability of the examination and must include:
- Patient demographics
- Study date and time
- Accession or study number
- Referring physician details
Accurateentifiers are essential for follow-up, comparison, audit, and medico-legal review.
Clinical History / Indication Section
Best practices include:
- Concise documentation focused on the reason for examination
- Inclusion of relevant symptoms, laboratory findings, or prior imaging
- Avoidance of unrelated or speculative clinical details
This section contextualizes imaging findings and improves diagnostic relevance.
Technique / Protocol Section
For USG abdomen, the technique section should document:
- Patient positioning during examination
- Transducer type and frequency range
- Real-time scanning methodology
- Use of Doppler evaluation, if performed
This section defines the technical scope and limitations of the study.
Findings Section – Organ/System-Wise Reporting
The findings section is the core diagnostic component and must follow objective reporting principles.
Best practices include:
- Describing observations before interpretation
- Reporting each organ separately
- Explicitly stating normal findings
- Describing abnormalities using size, echotexture, margins, and precise location
Commonly documented structures include:
- Liver
- Gallbladder and biliary tree
- Pancreas
- Spleen
- Kidneys
- Urinary bladder
- Major abdominal vessels
- Peritoneal cavity
Impression / Conclusion Section
The impression should:
- Summarize key imaging findings concisely
- Use conservative, non-definitive language
- Include differential considerations when appropriate
- Avoid diagnostic overstatement beyond imaging capability
This section guides clinicians while maintaining medico-legal safety.
Limitations of the Study
Limitations must be documented whenever applicable to ensure transparency.
Common examples include:
- Bowel gas obscuration
- Patient body habitus
- Suboptimal acoustic window
- Incomplete visualization of specific organs
Recommendations & Follow-Up (If Applicable)
Recommendations should be:
- Clinically appropriate and justified
- Non-directive and conservative in tone
- Clearly separated from diagnostic conclusions
Normal USG Abdomen Report Format (Sample)
Findings:
The liver is normal in size with homogeneous echotexture. No focal lesion isentified. Gallbladder is well distended with normal wall thickness. No calculi or sludge noted. Common bile duct is within normal limits. Pancreas, spleen, kidneys, and urinary bladder appear normal. No free fluid is seen.
Impression:
Normal ultrasonography of the abdomen.
Abnormal USG Abdomen Report Format (Sample)
Findings:
The liver appears mildly enlarged with altered echotexture. Gallbladder demonstrates an echogenic focus with posterior acoustic shadowing. Common bile duct is within normal caliber. Mild free fluid is noted in the pelvis.
Impression:
Ultrasonographic findings as described above. Clinical correlation is advised.
How Drlogy Radiology Reporting Software Standardizes These Report Formats
Clinically relevant standardization mechanisms include:
- Template-driven organ-wise reporting
- Impression safety controls to avoid overstatement
- Uniform formatting across imaging modalities
- AI-assisted draft generation from imaging workflows
- Audit-ready structured documentation
No pricing, promotional language, or call-to-action elements are included in clinical reporting.
10 Key Clinical Guidelines for an Effective USG Abdomen Report Format
- Maintain a consistent section order
- Document all evaluated organs
- Explicitly state normal findings
- Use standardized terminology
- Avoid speculative language
- Separate findings from impressions
- Document limitations clearly
- Verify patiententifiers
- Keep impressions concise
- Support longitudinal comparison
Adherence to these guidelines improves accuracy, efficiency, and medico-legal protection.
Common Reporting Errors to Avoid
- Omission of organ documentation
- Over-interpretation of equivocal findings
- Inconsistent terminology
- Failure to document limitations
- Non-standard impression phrasing
Medico-Legal Considerations in Radiology Reporting
Key medico-legal principles include:
- Complete and accurate documentation
- Use of conservative diagnostic language
- Clear accountability of reporting radiologist
- Documentation of study limitations
- Audit and peer-review readiness
- Secure record retention
- Consistency with accepted reporting standards
Structured Reporting vs Narrative Reporting
| Aspect | Structured Reporting | Narrative Reporting |
|---|---|---|
| Consistency | High | Variable |
| Audit readiness | Strong | Limited |
| Efficiency | Optimized | Operator dependent |
Role of Technology in Radiology Reporting
Technology supports radiology reporting through:
- PACS and RIS integration
- Voice dictation combined with structured templates
- AI-assisted formatting and consistency checks
- RIS-based structured reporting modules
- Modality-specific reporting software
Why High-Volume Radiology Centers Prefer Software-Based Reporting Formats
Operational advantages include:
- Reduced report turnaround time
- Improved quality assurance
- Consistency across multiple radiologists
- Scalability of reporting operations
- Improved audit readiness
- Reduced reporting errors
- Standardized documentation across modalities
Frequently Asked Questions (FAQs)
What is the standard structure of a USG abdomen report format?
A standardized sequence including patient details, technique, findings, impression, and limitations.
Should normal organs be explicitly documented?
Yes. Explicit documentation improves clarity, follow-up comparison, and medico-legal safety.
How detailed should the impression be?
Concise, summary-focused, and conservative, reflecting imaging findings only.
Is structured reporting mandatory?
Not mandatory, but strongly preferred in professional radiology practice.
Does software-based reporting replace clinical judgment?
No. Software supports consistency and completeness while preserving radiologist expertise.
Key Takeaways for Radiology Professionals
- Consistent structure improves diagnostic reliability
- Structured formats reduce omission and variability
- Conservative impressions protect professional integrity
- Technology enhances, not replaces, clinical expertise
Expert Picks
Final Conclusion
A standardized USG abdomen report format is fundamental to accurate clinical communication, patient safety, and medico-legal protection in modern radiology practice.
Structured reporting systems, when aligned with real-world workflows, enable consistency in high-volume environments and uphold professional standards while fully respecting the radiologist’s clinical judgment and responsibility.