Drlogy
Healthcare organization
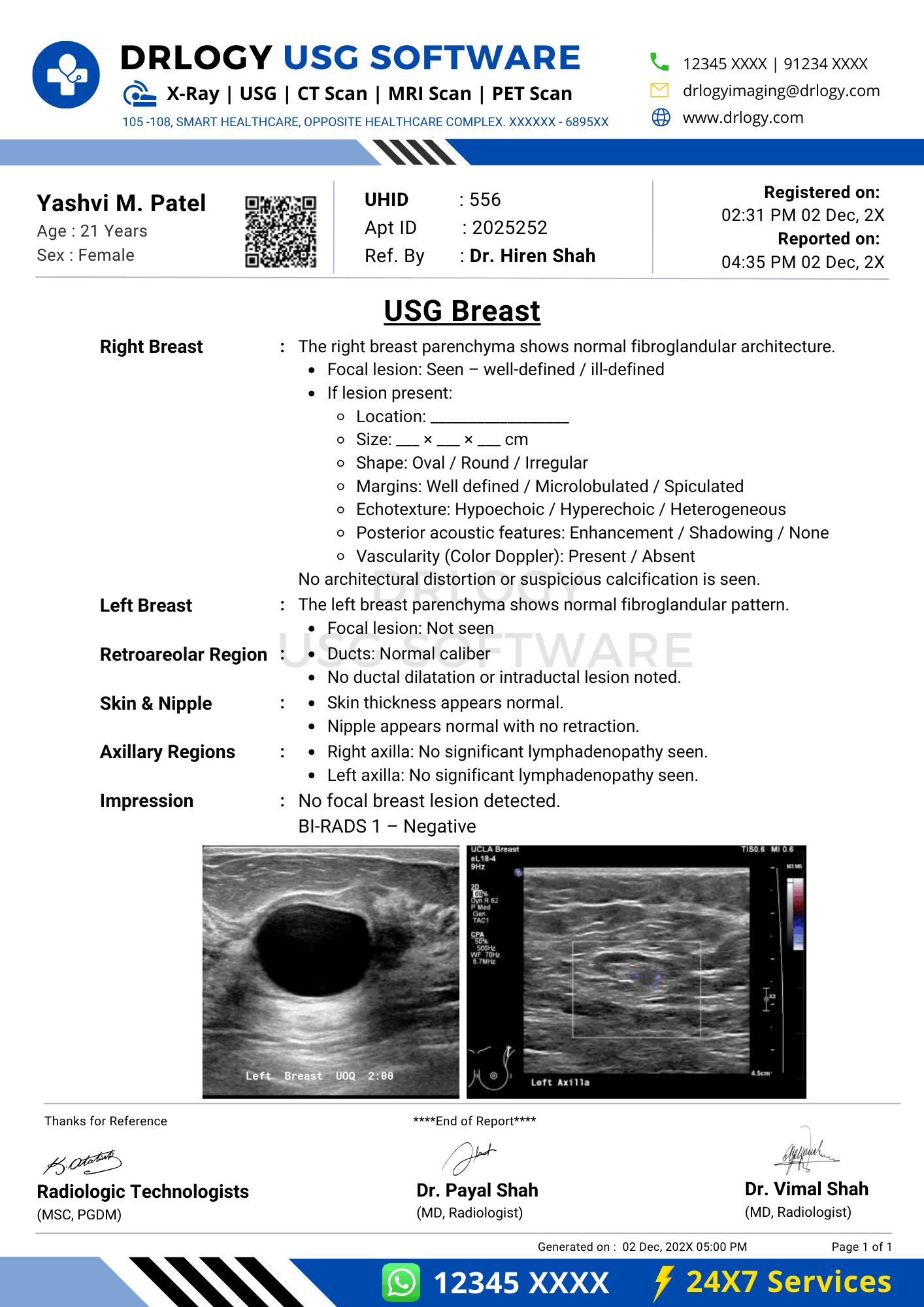
USG Breast Report Format for Radiologists
What Is a USG Breast Report Format?
A USG breast report format is a standardized professional framework for documenting ultrasonographic evaluation of breast tissue using precise anatomical, morphological, and sonographic descriptors.
It serves as a formal clinical communication tool supporting diagnosis, referrals, follow-up, inter-modality correlation, and longitudinal comparison across time.
It is a medico-legal document defining examination scope, technical adequacy, objective findings, conservative interpretation, and documented limitations aligned with accepted breast imaging standards.
Check:
Explore the Best AI-Based Ultrasound Reporting Software for Radiologists
Clinical Importance of a Standardized USG Breast Report Format
- Diagnostic clarity by enforcing structured documentation of lesion morphology, location, size, echogenicity, margins, posterior features, and vascularity.
- Inter-doctor communication through uniform terminology understood by radiologists, surgeons, oncologists, and referring clinicians.
- Reporting consistency across multiple radiologists, serial follow-up studies, and high-volume breast imaging workflows.
- Patient safety by minimizing omission of critical descriptors required for accurate risk stratification and follow-up planning.
- Medico-legal protection by ensuring objective documentation, standardized impressions, and explicit limitation statements.
A standardized USG breast report format improves interpretive reliability and audit readiness.
Why Manual Reporting Often Fails to Maintain Standardization at Scale
- Inter-radiologist variability in lesion description, BI-RADS terminology usage, and impression phrasing.
- Missed sections in high-volume settings such as axillary assessment, posterior acoustic features, or comparison with prior imaging.
- Terminology inconsistency leading to ambiguous lesion characterization and follow-up confusion.
- Audit challenges due to narrative reports lacking structured fields for quality review and medico-legal evaluation.
Structured reporting improves completeness, reproducibility, and medico-legal robustness.
Indications for USG Breast
- Palpable breast lump evaluation
- Breast pain or focal tenderness assessment
- Evaluation of dense breasts
- Characterization of mammographic findings
- Follow-up of known lesions
- Axillary lump assessment
- Screening in selected clinical contexts
Indications guide protocol selection and reporting emphasis.
Pre-Examination Details to Be Documented
- Patiententifiers including name, age, unique, accession number, study date and time.
- Referral details including referring clinician and clinical indication.
- Clinical notes including symptoms, duration, prior imaging, surgical history, and relevant risk factors if provided.
- Preparation status including patient positioning and comfort considerations.
- Safety checks including correct patient verification and laterality confirmation.
How Reporting Software Ensures Complete Pre-Examination Documentation
- Mandatory field enforcement for indication, laterality, and comparison status.
- Safety checklist compliance standardizing patiententification and side verification.
- Clinical note traceability linking referral information with imaging findings.
- Implementation example: Drlogy Radiology Reporting Software provides structured USG breast templates with compulsory lesion descriptor fields.
Standard Sections of a USG Breast Report Format
- Patient & Study Information
- Clinical History / Indication
- Technique / Protocol
- Findings (breast and axilla)
- Impression / Conclusion
- Limitations of the Study
- Recommendations & Follow-Up (if applicable)
Patient & Study Information Section
This section ensures traceability and accountability:
- Patient demographics andentifiers
- Study date, time, and accession number
- Referring clinician details
- Examination name and laterality
- Comparison with prior imaging when available
Clinical History / Indication Section
- Presenting complaint and duration
- Side of symptoms
- Relevant prior imaging or intervention
- Known breast disease history if provided
Documentation must remain concise and clinically relevant.
Technique / Protocol Section
- Positioning: supine or oblique with ipsilateral arm raised.
- Approach: high-frequency linear transducer examination.
- Coverage: systematic radial and anti-radial scanning of breast tissue.
- Axillary evaluation: assessment of lymph nodes when indicated.
- Doppler usage: documentation when vascularity assessment is performed.
Technique documentation defines examination adequacy and interpretive confidence.
Findings Section – Organ/System-Wise Reporting
Breast Parenchyma
- Echotexture and background pattern
- Symmetry comparison
Lesion Description
- Location by clock face and distance from nipple
- Size in three dimensions
- Shape and orientation
- Margin characteristics
- Echogenicity
- Posterior acoustic features
- Calcifications if visualized
- Associated architectural distortion
Axilla
- Lymph node morphology
- Cortical thickness
- Hilum status
Objective description must separate observed features from interpretation.
Impression / Conclusion Section
- Concise summary of significant findings
- Use conservative, standardized terminology
- BI-RADS category assignment where appropriate
- Avoid definitive diagnostic claims
Limitations of the Study
- Dense fibroglandular tissue
- Limited acoustic window
- Patient discomfort or motion
- Operator-dependent factors
Explicit limitation documentation is essential for medico-legal clarity.
Recommendations & Follow-Up (If Applicable)
- Correlation with mammography when appropriate
- Interval follow-up imaging
- Tissue diagnosis consideration based on imaging features
Recommendations must remain conservative and protocol-aligned.
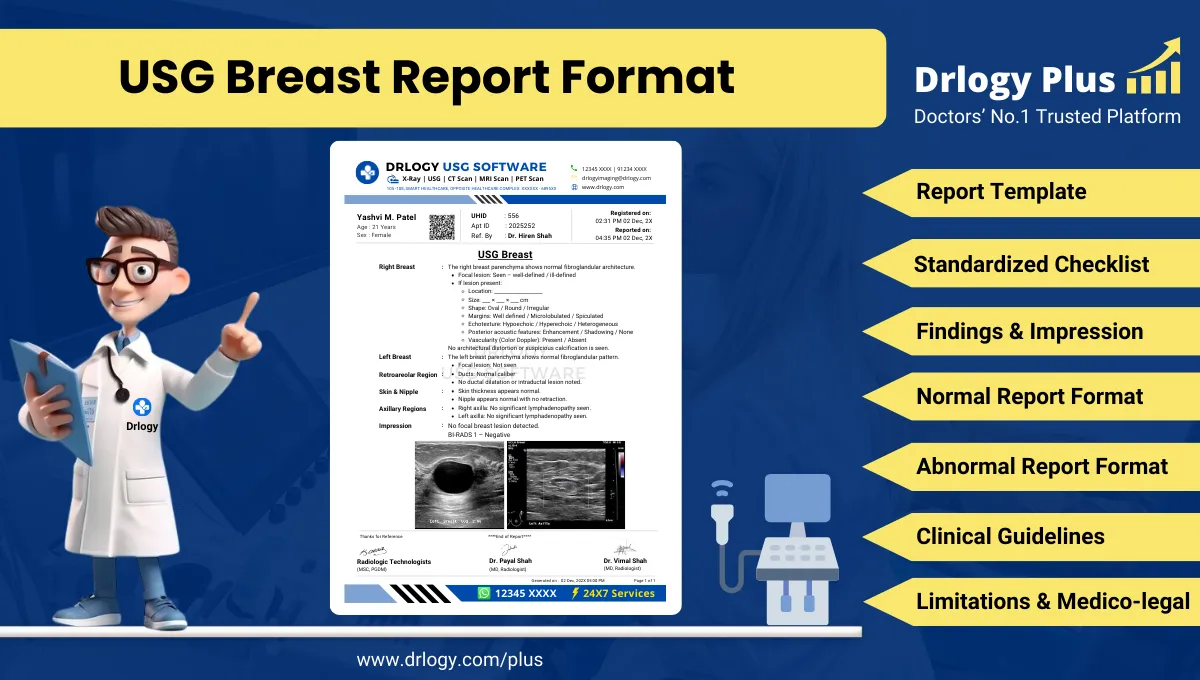
Normal USG Breast Report Format (Sample)
- Patient & Study Information:
- Patient: [Name], [Age]
- Study Date: [DD-MM-YYYY]
Examination: USG Breast
Clinical History / Indication:
Breast pain.
Technique / Protocol:
High-frequency ultrasound examination of bilateral breasts performed.
Findings:
Breast parenchyma appears homogeneous. No focal solid or cystic lesionentified. Axillary regions appear unremarkable.
Impression / Conclusion:
No sonographic abnormality detected.
Limitations:
No significant technical limitation noted.
Abnormal USG Breast Report Format (Sample)
- Patient & Study Information:
- Patient: [Name], [Age]
- Study Date: [DD-MM-YYYY]
Examination: USG Breast
Clinical History / Indication:
Palpable lump.
Technique / Protocol:
Ultrasound examination performed.
Findings:
A hypoechoic lesion is noted in the upper outer quadrant as described. Axillary lymph nodes show preserved morphology.
Impression / Conclusion:
Imaging findings as described. Correlation and further evaluation advised.
Limitations:
Assessment limited by dense parenchyma.
How Drlogy Radiology Reporting Software Standardizes These Report Formats
- Template-driven reporting ensuring complete lesion documentation
- Impression safety controls enforcing conservative wording
- Uniform formatting across breast imaging studies
- AI-enabled reporting assistance under radiologist verification
- Audit-ready documentation supporting quality assurance
10 Key Clinical Guidelines for an Effective USG Breast Report Format
- Document laterality clearly.
- Use standardized lesion descriptors.
- Measure lesions in three dimensions.
- Specify lesion location precisely.
- Assess posterior acoustic features.
- Evaluate axillary lymph nodes when indicated.
- Assign BI-RADS category appropriately.
- Separate findings from impression.
- Use conservative language.
- Document limitations explicitly.
Adherence improves reporting accuracy and medico-legal safety.
Common Reporting Errors to Avoid
- Incomplete lesion description
- Missing lesion measurements
- Omission of axillary assessment
- Overinterpretation of benign features
- Absence of limitation statements
Avoiding these errors strengthens report reliability.
Medico-Legal Considerations in Radiology Reporting
- Objective documentation of findings
- Use of standardized terminology
- Conservative impression language
- Explicit limitation statements
- Clear accountability
- Audit readiness
- Appropriate disclaimers
Structured Reporting vs Narrative Reporting
| Aspect | Structured | Narrative |
|---|---|---|
| Completeness | Protocol-based | Variable |
| Consistency | High | Operator dependent |
| Audit readiness | Strong | Limited |
| Efficiency | Optimized | Variable |
| Legal safety | Enhanced | Variable |
Role of Technology in Radiology Reporting
- PACS and RIS integration
- Voice dictation with templates
- AI-assisted formatting
- RIS-based structured templates
- Breast imaging workflow tools
Technology enhances consistency without replacing professional judgment.
Why High-Volume Radiology Centers Prefer Software-Based Reporting Formats
- Faster turnaround time
- Improved quality assurance
- Multi-radiologist consistency
- Scalable workflows
- Reduced omission errors
- Standardized BI-RADS usage
- Enhanced medico-legal protection
Frequently Asked Questions (FAQs)
What defines a standard USG breast report format?
A structured format documenting lesion descriptors, impression, BI-RADS category, and limitations using standardized terminology.
Is BI-RADS mandatory in breast ultrasound reporting?
BI-RADS categorization is recommended when lesion characterization is performed.
How should indeterminate lesions be reported?
Using objective descriptors with conservative impression and appropriate follow-up recommendations.
Why are limitations important in breast ultrasound reports?
They define reduced sensitivity and support medico-legal defensibility.
Key Takeaways for Radiology Professionals
- Use standardized structure for every USG breast examination.
- Document lesion morphology comprehensively.
- Maintain conservative impression language.
- Explicitly state limitations.
Consistent structured reporting improves diagnostic communication and medico-legal safety.
Expert Picks
Final Conclusion
A standardized USG breast report format is essential for accurate breast imaging communication, reliable follow-up planning, and medico-legal protection in clinical practice.
Structured reporting software supports consistency, completeness, and conservative interpretation while aligning with real-world radiology workflows and established professional standards.