Drlogy
Healthcare organization
USG Shoulder Report Format for Radiologists
What Is a USG Shoulder Report Format?
A USG shoulder report format is a standardized professional structure for documenting ultrasonographic assessment of the shoulder joint and periarticular soft tissues.
It serves as a clinical communication tool supporting diagnosis, referral, follow-up, and comparison with prior musculoskeletal imaging.
It is a medico-legal document defining examination scope, technical adequacy, objective findings, conservative interpretation, and documented limitations.
Check:
Explore the Best AI-Based Ultrasound Reporting Software for Radiologists
Clinical Importance of a Standardized USG Shoulder Report Format
- Diagnostic clarity through systematic evaluation of rotator cuff tendons, biceps tendon, bursae, joint recesses, and periarticular soft tissues.
- Inter-doctor communication using uniform musculoskeletal terminology understood by radiologists, orthopedicians, sports medicine specialists, and rheumatologists.
- Reporting consistency across serial examinations, multiple operators, and high-volume musculoskeletal practices.
- Patient safety by reducing missed assessment of critical structures such as supraspinatus tendon, biceps tendon sheath, and subacromial-subdeltoid bursa.
- Medico-legal protection through objective description, conservative impression wording, and explicit documentation of study limitations.
A standardized report format improves reproducibility, audit readiness, and longitudinal comparability in shoulder ultrasound reporting.
Why Manual Reporting Often Fails to Maintain Standardization at Scale
- Inter-radiologist variability in describing tendon echotexture, partial-thickness tears, and bursitis severity.
- Missed sections in high-volume settings such as incomplete evaluation of posterior cuff or dynamic impingement assessment.
- Terminology inconsistency leading to ambiguous communication regarding tendinopathy, tears, or inflammatory changes.
- Audit challenges because free-text narrative reports are difficult to benchmark and quality-check.
Software-assisted structured reporting supports completeness and uniformity without limiting professional judgment.
Indications for USG Shoulder
- Shoulder pain evaluation
- Suspected rotator cuff pathology
- Limited range of motion or impingement symptoms
- Soft tissue swelling around the shoulder
- Suspected biceps tendon pathology
- Follow-up of known inflammatory or degenerative shoulder conditions
A focused indication guides examination protocol and reporting emphasis.
Pre-Examination Details to Be Documented
- Patiententifiers including name, age, sex, unique, accession number, study date, and time.
- Referral details including referring clinician and clinical query.
- Clinical notes including pain location, duration, trauma history, and prior imaging if available.
- Preparation status including patient positioning and cooperation.
- Safety checks including patient verification and correct side confirmation.
How Reporting Software Ensures Complete Pre-Examination Documentation
- Mandatory field enforcement for indication, laterality, and examination scope.
- Safety checklist compliance ensuring correct patient and sideentification.
- Clinical note traceability linking referral information with imaging findings.
- Implementation example: Drlogy Radiology Reporting Software provides structured musculoskeletal templates with compulsory shoulder assessment fields.
Standard Sections of a USG Shoulder Report Format
- Patient & Study Information
- Clinical History / Indication
- Technique / Protocol
- Findings (structure-wise shoulder assessment)
- Impression / Conclusion
- Limitations of the Study
- Recommendations & Follow-Up (if applicable)
Patient & Study Information Section
This section ensures traceability and accountability:
- Patient demographics andentifiers
- Study date, time, and accession number
- Referring clinician details
- Examination name and laterality
- Comparison with prior imaging if available
Clinical History / Indication Section
- Presenting symptoms and duration
- Side involved
- History of trauma, overuse, or inflammatory disease
- Relevant prior interventions or imaging
Documentation should remain concise and clinically relevant.
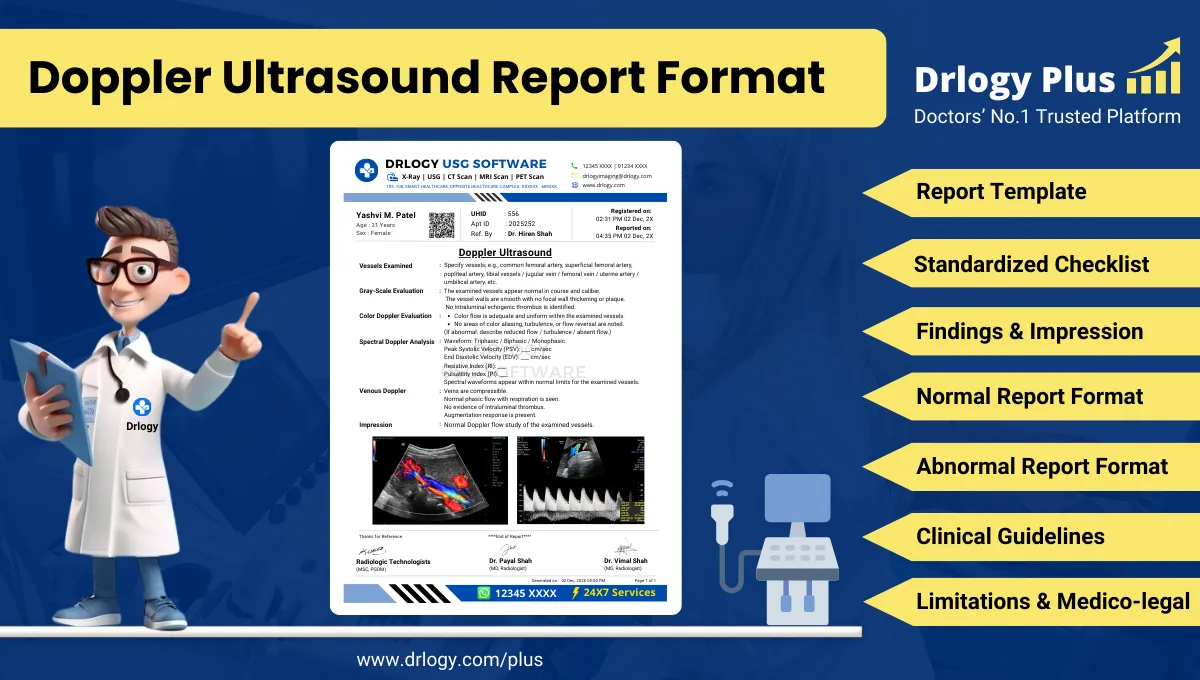
Technique / Protocol Section
- Positioning: seated or supine with arm positioned to optimize tendon visualization.
- Approach: high-frequency linear transducer examination.
- Views: anterior, lateral, superior, and posterior shoulder compartments.
- Dynamic assessment: real-time evaluation during arm movement when indicated.
- Doppler usage: documented when assessing hyperemia or inflammatory changes.
Technique documentation establishes examination adequacy and interpretive confidence.
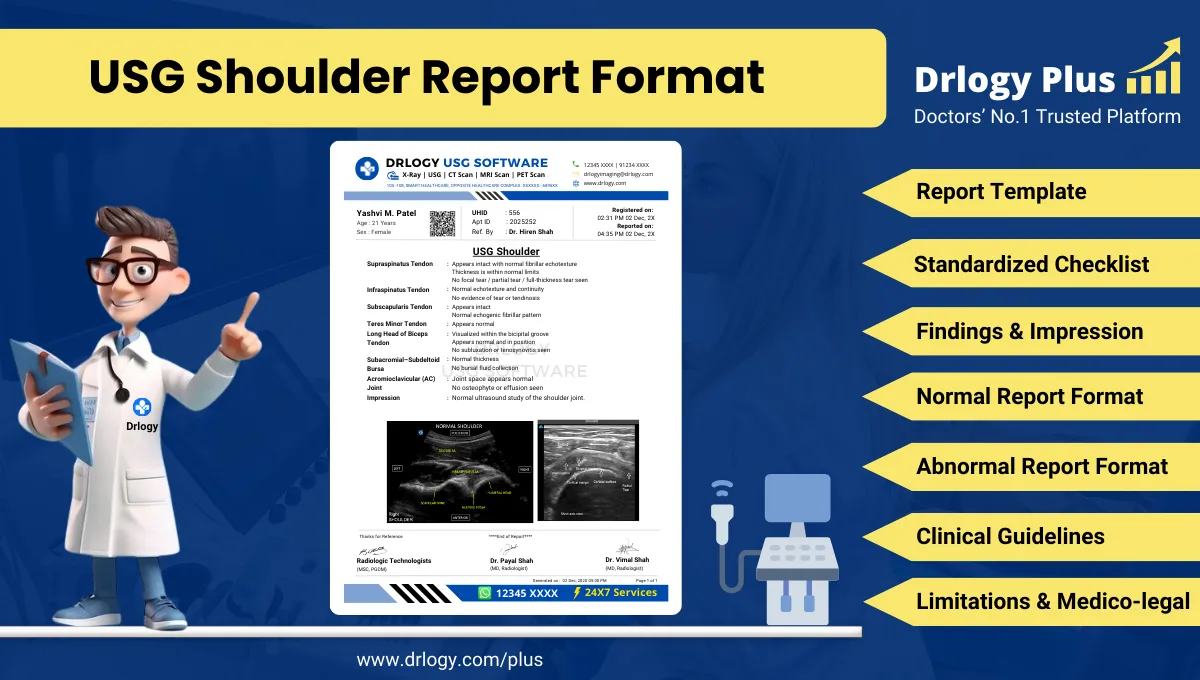
Findings Section – Organ/System-Wise Reporting
Biceps Tendon
- Position within bicipital groove
- Echotexture and continuity
- Effusion within tendon sheath
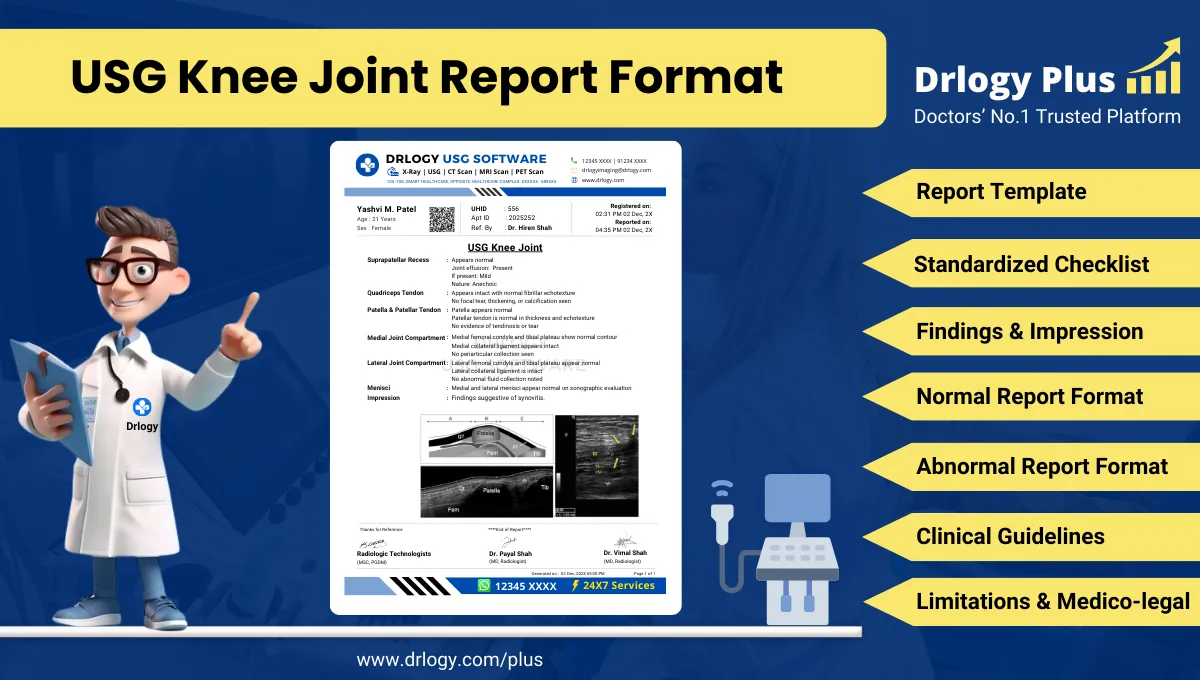
Supraspinatus Tendon
- Thickness and echotexture
- Focal hypoechoic areas or defects
- Calcific foci if present
Infraspinatus and Teres Minor Tendons
- Fiber continuity
- Tendon thickness and echogenicity
Subscapularis Tendon
- Integrity and dynamic stability
- Associated biceps tendon relationship
Subacromial-Subdeltoid Bursa
- Presence or absence of fluid
- Bursal thickening
Glenohumeral Joint Recesses
- Joint effusion
- Synovial hypertrophy
Objective description must clearly differentiate normal from abnormal findings.
Impression / Conclusion Section
- Concise summary of principal abnormalities
- Conservative, non-definitive language
- Avoidance of etiological or prognostic overstatement
- Recommendation for clinical correlation
Limitations of the Study
- Limited visualization of deep intra-articular structures
- Operator dependency
- Restricted patient movement
- Acoustic shadowing from bone
Explicit documentation supports medico-legal clarity.
Recommendations & Follow-Up (If Applicable)
- Clinical correlation with symptoms
- Follow-up imaging when appropriate
- MRI correlation for comprehensive intra-articular evaluation
Recommendations must remain conservative and appropriate.
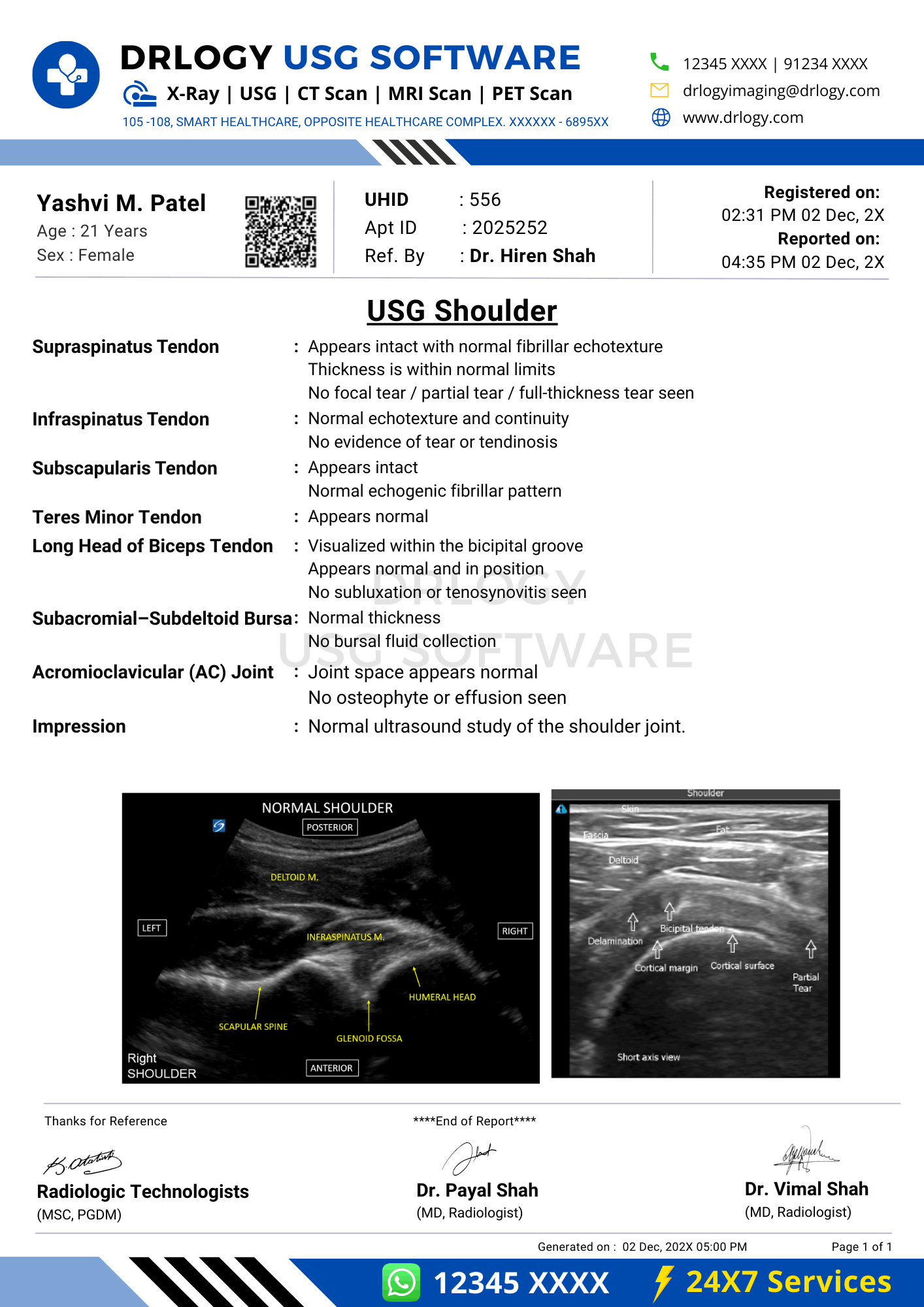
Normal USG Shoulder Report Format (Sample)
- Patient & Study Information:
- Patient: [Name], [Age]
- Study Date: [DD-MM-YYYY]
Examination: USG Shoulder
Clinical History / Indication:
Shoulder pain.
Technique / Protocol:
Ultrasound examination of the shoulder performed using high-frequency transducer.
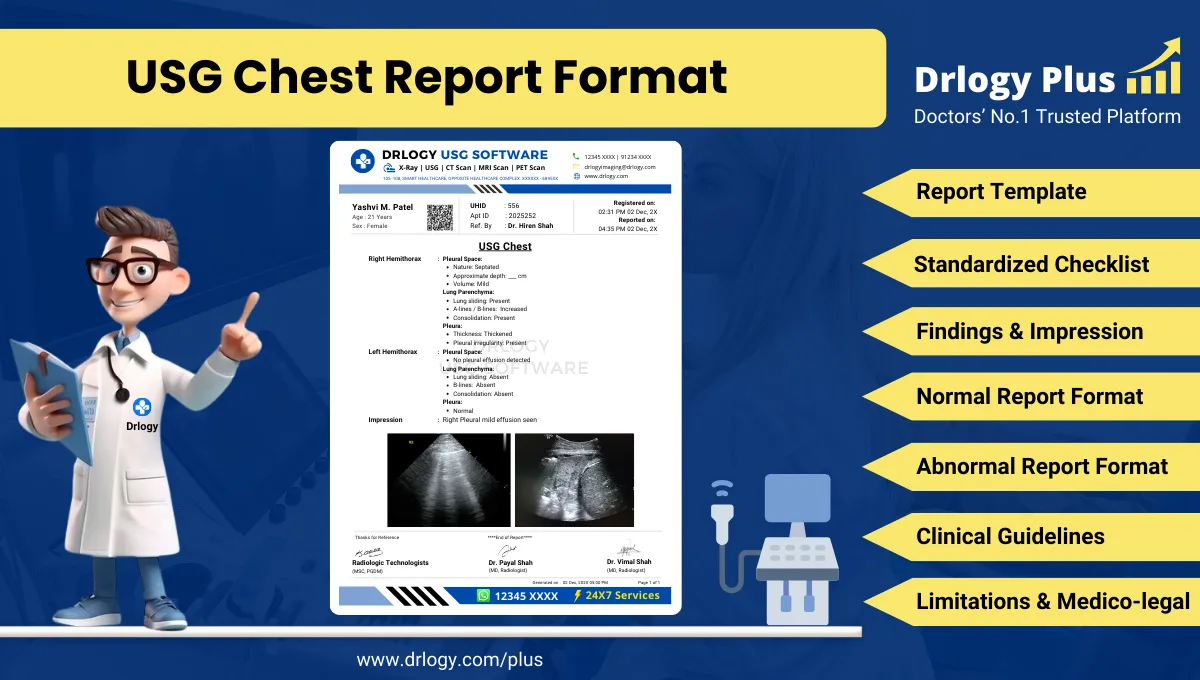
Findings:
Biceps tendon is normally positioned within the bicipital groove. Rotator cuff tendons appear intact with normal echotexture. No bursal fluid or joint effusion is seen.
Impression / Conclusion:
No significant sonographic abnormality detected in the shoulder.
Limitations:
No significant technical limitation noted.
Abnormal USG Shoulder Report Format (Sample)
Patient & Study Information: Patient: [Name], [Age] - Study Date: [DD-MM-YYYY]
Examination: USG Shoulder
Clinical History / Indication:
Pain and restricted movement.
Technique / Protocol:
Ultrasound examination performed.
Findings:
Supraspinatus tendon shows focal hypoechoic area suggestive of tendinopathy. Mild subacromial-subdeltoid bursal fluid is noted.
Impression / Conclusion:
Sonographic findings as described. Clinical correlation is advised.
Limitations:
Assessment limited by patient discomfort.
How Drlogy Radiology Reporting Software Standardizes These Report Formats
- Template-driven reporting ensuring systematic shoulder structure documentation
- Impression safety controls enforcing conservative language
- Uniform formatting across musculoskeletal examinations
- AI-enabled reporting assistance under radiologist supervision
- Audit-ready documentation supporting quality assurance
10 Key Clinical Guidelines for an Effective USG Shoulder Report Format
- Document laterality clearly.
- Assess all rotator cuff tendons systematically.
- Evaluate biceps tendon position and sheath.
- Document bursal findings objectively.
- Use standardized anatomical terminology.
- Separate findings from impression.
- Avoid definitive intra-articular diagnoses.
- Document dynamic assessment when performed.
- State limitations explicitly.
- Maintain consistent report structure.
Adherence improves reporting accuracy and medico-legal safety.
Common Reporting Errors to Avoid
- Omission of posterior cuff evaluation
- Vague tendon descriptions
- Failure to document laterality
- Overinterpretation of ultrasound findings
- Missing limitation statements
Avoidance of these errors strengthens report reliability.
Medico-Legal Considerations in Radiology Reporting
- Objective documentation of findings
- Standardized terminology usage
- Conservative impression language
- Explicit limitation statements
- Clear accountability
- Audit-ready structure
- Appropriate disclaimers
Structured Reporting vs Narrative Reporting
| Aspect | Structured | Narrative |
|---|---|---|
| Completeness | High | Variable |
| Consistency | Standardized | Operator dependent |
| Audit readiness | Strong | Limited |
| Efficiency | Optimized | Variable |
| Legal safety | Enhanced | Variable |
Role of Technology in Radiology Reporting
- PACS and RIS integration
- Voice dictation
- AI-assisted formatting
- RIS-based structured templates
- Musculoskeletal workflow tools
Technology enhances consistency without replacing professional judgment.
Why High-Volume Radiology Centers Prefer Software-Based Reporting Formats
- Faster turnaround time
- Improved quality assurance
- Multi-radiologist consistency
- Scalability across MSK studies
- Reduced omission errors
- Standardized documentation
- Enhanced medico-legal protection
Frequently Asked Questions (FAQs)
What defines a standard USG shoulder report format?
A structured format documenting rotator cuff, biceps tendon, bursae, impression, and limitations using standardized musculoskeletal terminology.
Can ultrasound diagnose all shoulder pathologies?
Ultrasound evaluates accessible soft tissues and should be correlated with MRI for comprehensive intra-articular assessment.
How should tendon abnormalities be reported?
By objective description of echotexture, continuity, and location without definitive etiological conclusions.
Why are limitations essential in shoulder ultrasound reports?
They define modality constraints and support medico-legal defensibility.
Key Takeaways for Radiology Professionals
- Use standardized structure for every shoulder ultrasound.
- Document all rotator cuff tendons systematically.
- Maintain conservative impression wording.
- Explicitly state technical limitations.
Consistent structured reporting improves musculoskeletal ultrasound reliability.
Expert Picks
Final Conclusion
A standardized USG shoulder report format is essential for accurate musculoskeletal imaging communication, reliable follow-up, and medico-legal safety in daily radiology practice.
Structured reporting software supports consistency, completeness, and conservative interpretation while aligning with real-world radiology workflows and professional standards.